-
 Hanover
15.3k"South Dakota’s coronavirus cases have begun to soar after its governor steadfastly refused to mandate a quarantine.
Hanover
15.3k"South Dakota’s coronavirus cases have begun to soar after its governor steadfastly refused to mandate a quarantine.
The number of confirmed cases in the state has risen from 129 to 988 since April 1 — when Gov. Kristi Noem criticized the “draconian measures” of social distancing to stop the spread of the virus in her state.
Noem had criticized the quarantine idea as “herd mentality, not leadership” during a news conference, adding, “South Dakota is not New York.”"
Yall need to bring back public hanging of public officials. — StreetlightX
And their deaths per million is now 8, 2nd lowest in the nation. South Dakota isn't New York. There are 10.7 people per square mile in SD, compared to 411.2 in NY (70,826 per square mile in Manhattan). This is to say that South Dakotans practice more social distancing on an average day than a New Yorker practices on total lock down. It's not a one size fits all, which is why the individual governors are given the ability to decide the best course of action. -
Hanover
15.3kWhat's the right wing of the Repub party's excuse? — Baden
Can't say. My excuse is is that I don't interact with the elderlies, so I can't do any harm, so set me free. I'm also running out of room from all this toilet paper I've got.
I'm gonna go get an MD or something so I can control the damn world. Dr. Hanover will be an emancipator, not a regulator. He won't be spittin no viruses, just rhymes. -
 Deleteduserrc
2.8kMy company just laid off a bunch of people. Luckily, I still have my job. The CEO took a 20% paycut. However, after reading a few articles, found this passage. It went uncommented on, in the comment sections, so maybe I just don't have the finance/business background to adequately contextualize it, but it seems shady af to me. Anyone have any insight to this, and whether it's as bad a thing as it looks?
Deleteduserrc
2.8kMy company just laid off a bunch of people. Luckily, I still have my job. The CEO took a 20% paycut. However, after reading a few articles, found this passage. It went uncommented on, in the comment sections, so maybe I just don't have the finance/business background to adequately contextualize it, but it seems shady af to me. Anyone have any insight to this, and whether it's as bad a thing as it looks?
On Feb. 18, when Wex stock was trading above $220 per share, company President and CEO Melissa Smith exercised an option to buy 8,056 shares of Wex stock at a discounted price of $77.20, then immediately sold 15,556 shares at $223.19 per share for a total cash-out of just under $3.5 million, according to a filing with the U.S. Securities and Exchange Commission. — Portland Press Herald -
Deleteduserrc
2.8kThat's gorgeous! What country/region are you in?
To assuage any fears about my well-being, I do get out most days. Lucky enough to live near a tranquil park w/ altitude which overlooks Southern Maine as it stretches north til the foothills, and past that to the mountains. And a slow 2.5 hour walk will let me circle the city and stop at the park on the other end, which looks out onto the ocean. However, it's not isolated; at either park, there are usually a fair number of others around. An old cemetery nearby works for outdoors isolation, but, of course, its a cemetery. Which I'm ok with, but you can't really ignore the fact there's a bunch of civil war vets a few feet down. -
 Pfhorrest
4.6kSo the Paycheck Protection Program ran out of money this morning. My semi-former employer was counting on that to keep his business afloat, and I was counting on that in turn to have a job to come back to before my enhanced unemployment runs out.
Pfhorrest
4.6kSo the Paycheck Protection Program ran out of money this morning. My semi-former employer was counting on that to keep his business afloat, and I was counting on that in turn to have a job to come back to before my enhanced unemployment runs out.
It sounds like a bill to re-fund it is already in the works, but the new funds are expected to run out just as quickly, and apparently Democrats are holding up the bill (!?), though I can’t find any good information on why.
ETA: It appears Democrats want more hospital funding and better access to the money for small lenders, and Trump sounds pretty okay with that, it’s just senate Republicans who want to leave that out. -
 Streetlight
9.1kYet the point is that a great deal of those infections - and correponding deaths - were likely preventable. They need not have happened.
Streetlight
9.1kYet the point is that a great deal of those infections - and correponding deaths - were likely preventable. They need not have happened. -
 Changeling
1.4kWhat country/region are you in? — csalisbury
Changeling
1.4kWhat country/region are you in? — csalisbury
From what I can ascertain: West Anglia. -
 Benkei
8.1kI'm sure it was done legally but I don't see how yet. Prima facie it seems to be a breach of the holding period as described here: https://www.sec.gov/reportspubs/investor-publications/investorpubsrule144htm.html
Benkei
8.1kI'm sure it was done legally but I don't see how yet. Prima facie it seems to be a breach of the holding period as described here: https://www.sec.gov/reportspubs/investor-publications/investorpubsrule144htm.html -
Benkei
8.1kThanks. I actually started with the one before that. Looking into getting a kf94 mask now, which unfortunately may not be exported from Korea or Taiwan unless you're Korean or Taiwanese and live abroad.
Sucks monkey balls. -
 Isaac
10.3kIntroducing a new pattern that has no causal mechanism to significantly overlap (and thus displace) an existing pattern simply results in more deaths and no first-order reason to believe deaths will be lower when that pattern goes away. — boethius
Isaac
10.3kIntroducing a new pattern that has no causal mechanism to significantly overlap (and thus displace) an existing pattern simply results in more deaths and no first-order reason to believe deaths will be lower when that pattern goes away. — boethius
But it's not a pattern which has no causal mechanism to significantly overlap an existing pattern. Why do you think the government has sent out specific advice to vulnerable people? What biological mechanism do you think takes place to account for variation in disease course if not the ability of the immune system to respond? Viral load is certainly one factor, but it's unsure at this stage whether that's even a significant factor (one study says it could be, two other say it isn't, but those have yet to be peer reviewed).
So as things stand we're left with immune system response as being the only mechanism that has been reliably demonstrated to account for the variability in outcome. Meaning that literally everyone who experiences a poor outcome does so on account of a compromised immune response (except as I said, if the Lancet paper is right then very hight loads such as healthcare professionals are exposed to could be a factor too, but not for the general population).
So how do immune responses become compromised other than by underlying health conditions?
Likewise, most people at risk of respiratory illness will also not die this year nor people suffering from heart disease. — boethius
No, and most people who get Covid-19 won't die this year either. That's not the point. The point is that of those people who will die, a disproportionate amount will be drawn from that small group of people who were going to die from respiratory illness or heart disease. We're talking about quite small proportions in either case, so it's no good saying that only a very small proportion of those with underlying health conditions were going to die this year anyway. We know with great precision how many of those people were going to die this year anyway, its about 300,000 (the death rate minus deaths from accidents). So until the death rate from Covid-19 exceeds 300,000 you can't possibly say that the victims were not going to die anyway, simply on the basis of the numbers, you additionally need data on the overlap - or you need to wait for deaths occurring over a longer timescale - say a year, or you need a plausible mechanism of fatality which does no coincide with underlying health conditions.
People will continue to die of hear attacks for instance; there's no reason that Covid is killing people who really would die of a heart attack this year compared to people simply at risk of dying of a heart attack — boethius
Again, not to labour the point, but there absolutely is such a reason. People who are going to die from heart disease this year will disproportionately be in worse general health (specifically cardiovascular health) than those (from the same cohort) who were going to last more than a year. Death does not harvest randomly. Those who were ill enough to be likely to die this year from heart disease are more likely to die from Covid-19. That is why we see a disproportionate number of deaths in these categories.
maybe other second-order effects increase causal death mechanism, such as lung injury. — boethius
Again, not comparing like with like. If you're including (in your risk analysis) for Covid-19 potentially related deaths, then when comparing it to risks we know already, you have to do the same. Many illnesses have related tissue damage which causes morbidity later on, we don't include it in the death statistics for that condition - so why would we change our statistical approach for this particular condition?
Covid-19 may well be with us for some years, and if not this, then the next one. We have to manage it (and more importantly learn to cope with it psychologically) in a sustainable and consistent manner. I understand the impetus, but artificially making it sound more terrifying than it already is does not get people to act in the rational manner needed at times like these, nor is it healthy for the population in the long-run (not that the mental health of the population in the long run isn't already a lost cause - one might as well be holding back floodwater with a sieve) -
 ssu
9.8k
ssu
9.8k
You have two interpretations: a) Melissa wanted the cash from the options immediately. Many who get into the options program don't have any incentive to actually hold on to the stock, but treat it just a bonus like cash. Of course, the other way is to think that b) Melissa knew that the company was totally lost and verge of collapse and has absolutely no faith in the company.Anyone have any insight to this, and whether it's as bad a thing as it looks? — csalisbury -
 Jamal
11.8kPerhaps if folk post an image of where they isolate, it would be interesting to see how our experiences differ? — Punshhh
Jamal
11.8kPerhaps if folk post an image of where they isolate, it would be interesting to see how our experiences differ? — Punshhh
Right now I long for a garden like that. England?
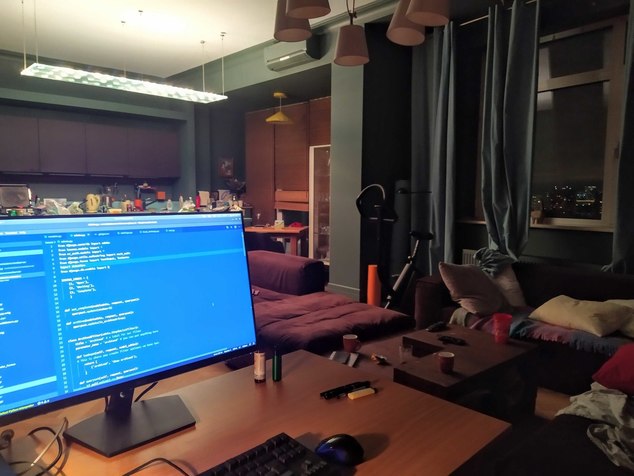
Isolation Station, Moscow. Pretty much the same as before to be honest, although now my wife is working from home as well, and we can't go out except for essentials. Out the window I can see for many miles across the city, places I cannot go.
Earlier this week, or maybe last week, the Moscow authorities introduced a pass system for travel. If you want to go anywhere in a car or by public transport, you need to get a special QR code from the local government web site. If the police catch you without one they'll fine you 5000 rubles.
Locals are generally derisive about this system, partly because it's been introduced in a rush and quite incompetently and chaotically. The web site crashed several times and the mayor immediately blamed foreign hackers--which I think convinced exactly nobody--and the police don't have scanning devices to check the QR codes, so they have to call back to base to confirm the code's validity. This has caused long queues at the metro stations, leading one journalist to caption a photo with "Stations of the Moscow metro are experiencing unprecedented DDoS attacks organized from abroad". I'm getting to like the Russian sense of humour.
EDIT: I really should clean up. -
 boethius
2.7kBut it's not a pattern which has no causal mechanism to significantly overlap an existing pattern. — Isaac
boethius
2.7kBut it's not a pattern which has no causal mechanism to significantly overlap an existing pattern. — Isaac
No, there's no causal mechanism that will cause significant overlap, unless by significant you mean measurable.
I've repeatedly said I have no problem with your claim we'd see an effect of people dying in the "otherwise would have died" category, but it's not a big effect.
Most of the risk categories, including respiratory, will continue to suffer from whatever they are at risk of.
What would make a significant overlap with people who really would have otherwise died I have outlined:
1. Early days with low numbers and cause and effect is not clear, the disease could be simply correlated with the other comorbities but not causal.
2. A disease that has enormous bias towards killing the terminally ill, but essentially no one else -- such as a hospital disease.
3. A super high mortality rate and completely out of control epidemic that has large overlaps with other "would be causes of death" simply due to killing so many people. For instance, many people dying in an Ebola outbreak are genuinely people who would have died anyways in the short term; so there's lot's of overlap but the effect is now small because total deaths are so high anyways -- doesn't do much for lowering attribution of death to the disease. — boethius
Being in an at-risk group increases your risk of dying if you get Covid, but the progression of Covid, in itself, does not significantly alter the nature of those risk groups going forward, such as culling the people that would actually die soon, without some mechanism -- a mechanism which is simply not there. Risk groups of Covid are very large groups we'd expect to be vulnerable, such as elderly, obese, diabetics, smokers, and so on.
I am not arguing with the fact there are groups more likely to die of Covid if they get infected. I am arguing with the idea that there will be a significant decrease in smokers dying because Covid preemptively removed smokers that would have otherwise died soon.
No, and most people who get Covid-19 won't die this year either. That's not the point. The point is that of those people who will die, a disproportionate amount will be drawn from that small group of people who were going to die from respiratory illness or heart disease. — Isaac
Exactly where we disagree.
Yes, the people who would otherwise die of respiratory disease are a small group.
But no, people dying from Covid are not drawn from this small group, but very large risk groups of which this group of people who actually die, or would have actually died, this year is a small subset.
Smoking, obesity, being old, are very large groups. Covid killing some people in those groups is just as random as other causal mechanisms that make these risk groups exist. Since the probability of death due to being a smoker is fairly small for the average smoker and the probability of death of Covid is fairly small, then we can essentially ignore intersection of "smokers dying of general risks of smoking" and "smokers dying of Covid".
If Covid killed all smokers, then yes there would be complete intersection and we could look forward to having less deaths relating to smoking; this would be the ebola example.
If Covid only targeted smokers in the terminally ill phase of lung cancer then again there's an intersection; the hospital disease case.
Likewise, if Covid was not a cause of disease but something everyone already had just scientists didn't know it, then it could easily be a false alarm that there's a new terrible disease; this would be the corollary-causation mixup.
But we know we can rule these things out.
Again, not comparing like with like. If you're including (in your risk analysis) for Covid-19 potentially related deaths, then when comparing it to risks we know already, you have to do the same. — Isaac
That's why I clearly make the distinction of respiratory illness decreasing after Covid because those people were culled from risk groups, and respiratory illness going down after Covid due to less pollution or other second order affects of Covid.
Our response to Covid is a massive systematic causal change to all sorts of things. So, it is definitely true we might see less respiratory deaths because of massive systemic changes to society; but it's a mistake to attribute that decrease to "people who would have otherwise died, but Covid got to them first and so they were not available to die in the existing death patterns we see".
However, we also know that the disease can cause long term lung damage, so it could be that we see this effect dominating the less pollution effect.
Point being, we cannot assume anything about these second order effects on face value. We can list effects, but we can't conclude which trend we will see nor conclude that our list of effects is exhaustive without some detailed model justification -- i.e. the opposite of face value.
We can be confident less pollution is good for lungs, and more lung damage is bad, but we can't know which will be the bigger effect, especially in a scenario where we don't find any effective treatment and everyone gets the disease.
We should also not confuse second order effects with primary effects of changing the makeup of risk groups in absolute terms as direct consequence of the disease killing some people.
As an aside, I did a lot of looking for the source of the "roughly double your existing annual risk", and found it in a search engine cache, so I didn't dream it. It's from a BBC article posting a graph from Imperial College analysis, but seems to be removed from the original article, I imagine because it give the impression that the risk of death for all age groups is completely unchanged by the pandemic, rather than it simply overlaying risk of death from Covid, if you become a case, onto of your existing risk in relation to the single risk dimension of age. Anyways, I'll upload it as it's an interesting pattern, but it's not needed for my above arguments to work. -
Changeling
1.4kVideo of a guy giving food to the homeless during the pandemic (but making sure to film it to get that praise and YouTube views/money).
-
Isaac
10.3kNo, there's no causal mechanism that will cause significant overlap, unless by significant you mean measurable. — boethius
Covid-19 kills people either by the lungs filling with fluid as a result of a failure of the immune system (sometimes from comorbid bacterial infection) or by exacerbating the effects of other conditions, particularly heart disease. Every single one of those mechanisms relies on an underlying health problem. If you know of some way Covid-19 applies a random element to the selection of fatalities, I'd be interested to hear it. As it stands, if you lined up 1000 people in order of healthiness and gave them all Covid-19, the one who will die will be drawn from the least healthy end. Likewise if you lined up all 70 million people in the country in order of healthiness, the 300,000 who are going to die this year (from disease) will be drawn from the least healthy end. It's the same cohort.
I don't know how else to explain this. There are 300,000 people who are so ill that they're going to die this year. You're suggesting that when these people get a Covid-19 infection, they're not significantly more likely to die from it then anyone else, that the deaths won't be drawn with any significant bias from this group.
Being in an at-risk group increases your risk of dying if you get Covid, but the progression of Covid, in itself, does not significantly alter the nature of those risk groups going forward, such as culling the people that would actually die soon — boethius
Of course it significantly alters the nature of the risk groups. So far 98% of Covid-19 deaths are from these risk groups, so if Covid-19 kills 20,000 people, then these risk groups will be 19,600 people smaller than they were beforehand. They are not like an exclusive club, they don't have a waiting list. If 19,600 people suddenly get removed from these groups, there's not a reserve cohort waiting to take their place. The 300,000 deaths are also drawn mainly from these cohorts. Again 300,000 is not a quota to be filled. If Death finds fewer people in his preferred selection group than normal he's not going to go looking elsewhere to bump up the numbers.
Smoking, obesity, being old, are very large groups. Covid killing some people in those groups is just as random as other causal mechanisms that make these risk groups exist. — boethius
No it isn't. Even within a risk group, the least healthy members of that risk group are more likely to die than the most healthy. There's no dice in our bodies that a virus gets to roll to see if it's going to kill us or not. It's a direct and unmediated consequence of the response of the immune system and the function of supporting organs. There's no roulette wheel involved. -
boethius
2.7kCovid-19 kills people either by the lungs filling with fluid as a result of a failure of the immune system (sometimes from comorbid bacterial infection) or by exacerbating the effects of other conditions, particularly heart disease. Every single one of those mechanisms relies on an underlying health problem. — Isaac
Nothing I have said contradicts this. -
Isaac
10.3kNothing I have said contradicts this. — boethius
Then where is the random mechanism? If you agree that it is failure of the immune response and supporting organs which leads to death, then it directly follows that those with the weakest immune systems and supporting organs will almost exclusively be the group from which fatalities will be drawn.
If you want to claim fatalities are drawn randomly from that group you need to describe the random mechanisms, so far all we have agreed on are non-random mechanisms directly related to health. -
boethius
2.7kNo it isn't. Even within a risk group, the least healthy members of that risk group are more likely to die than the most healthy. — Isaac
This is not true.
For this to be true, the "less healthy members" within a risk group need to somehow be far more likely to get infected to begin with. That is certainly not the case so far.
Furthermore, it would need to be the case that being particularly at risk of Covid within a risk group, means being particularly at risk of whatever makes up your risk group. It could be random genetic differences that make a person in a risk group, such as smoking, particularly at risk of Covid.
In other words, one could be a on the "healthy side" of a risk group, but particularly vulnerable to Covid due to some genetic difference that has no bearing on one's underlying condition. -
boethius
2.7kThen where is the random mechanism? — Isaac
The random mechanism is that we don't know who within a risk group is actually going to die this year, so taking people out of the group by another mechanism, such as Covid, doesn't change significantly the expected pattern of death from the existing risk. The randomness is due to a lack of knowledge at this stage; but there's no reason to expect Covid targets "the particularly unhealthy members of a risk group". -
Isaac
10.3kFor this to be true, the "less healthy members" within a risk group need to somehow be far more likely to get infected to begin with. — boethius
No they don't, because if everyone is equally likely to be infected then the liklihood of infection can be removed from the equation. It's only relevant if it biases fatality in the opposite direction. We're looking at whether fatalities are going to be significantly disproportionately drawn from certain groups. If 10% of all groups become infected, then we're dealing with 10% of the healthy cohort vs 10% of the least healthy cohort.
It could be random genetic differences that make a person in a risk group, such as smoking, particularly at risk of Covid. — boethius
Unless you're suggesting that there's some gene specific to the defense against Covid-19, then the only genetic component which might be relevant is one which affects the immune system in general. Such as defect would put you in the cohort from which the 300,000 yearly deaths are drawn.
The random mechanism is that we don't know who within a risk group is actually going to die this year, — boethius
Yes we do. It will (disproportionately) be the least healthy. Same as those most likely to die from Covid-19.
It might be different in a country whose disease-related deaths were mostly infections (like some developing countries) but not in the Western world. Our deaths are drawn overwhelmingly from heart disease and cancer. The exact same groups from which Covid-19 is drawing most of it's fatalities (with cancers being mostly the immune suppressing effects of treatment). -
boethius
2.7kNo they don't, because if everyone is equally likely to be infected then the liklihood of infection can be removed from the equation. — Isaac
No it can't, if you're trying to support the idea that Covid kills the "particularly unhealthy". Lot's of "particularly unhealthy" simply don't get the disease, so there will remain lot's of these "particularly unhealthy" around since they didn't get infected.
Unless you're suggesting that there's some gene specific to the defense against Covid-19, then the only genetic component which might be relevant is one which affects the immune system in general. Such as defect would put you in the cohort from which the 300,000 yearly deaths are drawn. — Isaac
I'm saying there's no reason to assume the variation of death and survival within a risk group is due to being "particularly unhealthy" within that group. It could be some other mechanism such as otherwise benign genetic differences, or then simply random variation such as where exactly the virus begins replicating in the body, that then dominates chances of death within a risk group.
Yes we do. It will (disproportionately) be the least healthy. Same as those most likely to die from Covid-19. — Isaac
As I've explained above, this is not a given assumption.
We cannot assume those that die from Covid are "least healthy" within their risk group.















Welcome to The Philosophy Forum!
Get involved in philosophical discussions about knowledge, truth, language, consciousness, science, politics, religion, logic and mathematics, art, history, and lots more. No ads, no clutter, and very little agreement — just fascinating conversations.
Categories
- Guest category
- Phil. Writing Challenge - June 2025
- The Lounge
- General Philosophy
- Metaphysics & Epistemology
- Philosophy of Mind
- Ethics
- Political Philosophy
- Philosophy of Art
- Logic & Philosophy of Mathematics
- Philosophy of Religion
- Philosophy of Science
- Philosophy of Language
- Interesting Stuff
- Politics and Current Affairs
- Humanities and Social Sciences
- Science and Technology
- Non-English Discussion
- German Discussion
- Spanish Discussion
- Learning Centre
- Resources
- Books and Papers
- Reading groups
- Questions
- Guest Speakers
- David Pearce
- Massimo Pigliucci
- Debates
- Debate Proposals
- Debate Discussion
- Feedback
- Article submissions
- About TPF
- Help
More Discussions
- Other sites we like
- Social media
- Terms of Service
- Sign In
- Created with PlushForums
- © 2026 The Philosophy Forum